

Normal Aortic Valve (I)
 A. Cephalad view of the aortic valve of a newborn shows delicate translucent cusps of roughly equal sizes, with equidistant commissures. In infancy, the aortic and pulmonic valves look similar and are identified primarily by their anatomic landmarks. As a function of age the aortic valve, becomes more opaque than the pulmonic valve, due to mechanically induced endocardial thickening associated with the higher pressures in the systemic circulation. B. Mild thickening of the leaflets occurs in adults, as shown in this front view of two aortic leaflets. The aortic root transitions into the cardiac muscle ate the fibrous skeleton. C. The semilunar valves are supported at the U-shaped attachment of the cusps to the root of the great arteries, with the commissures located superiorly. The lineae albae or lines of apposition (free edges) are more prominent in the aortic valve than in the pulmonic valve (B and C). In the older individual the apposition of the leaflets creates an area of thickening below the linea alba, which is called the closing edge. Between the closing edge and the linea alba, there is an oblong shaped depression called the lunula. The mid portion of the free edge (between the two commissures of a cusp) usually shows a nodular thickening, called the Nodulus of Arantius. Pathologic entities affecting the aortic valve may be congenital or acquired.
A. Cephalad view of the aortic valve of a newborn shows delicate translucent cusps of roughly equal sizes, with equidistant commissures. In infancy, the aortic and pulmonic valves look similar and are identified primarily by their anatomic landmarks. As a function of age the aortic valve, becomes more opaque than the pulmonic valve, due to mechanically induced endocardial thickening associated with the higher pressures in the systemic circulation. B. Mild thickening of the leaflets occurs in adults, as shown in this front view of two aortic leaflets. The aortic root transitions into the cardiac muscle ate the fibrous skeleton. C. The semilunar valves are supported at the U-shaped attachment of the cusps to the root of the great arteries, with the commissures located superiorly. The lineae albae or lines of apposition (free edges) are more prominent in the aortic valve than in the pulmonic valve (B and C). In the older individual the apposition of the leaflets creates an area of thickening below the linea alba, which is called the closing edge. Between the closing edge and the linea alba, there is an oblong shaped depression called the lunula. The mid portion of the free edge (between the two commissures of a cusp) usually shows a nodular thickening, called the Nodulus of Arantius. Pathologic entities affecting the aortic valve may be congenital or acquired.
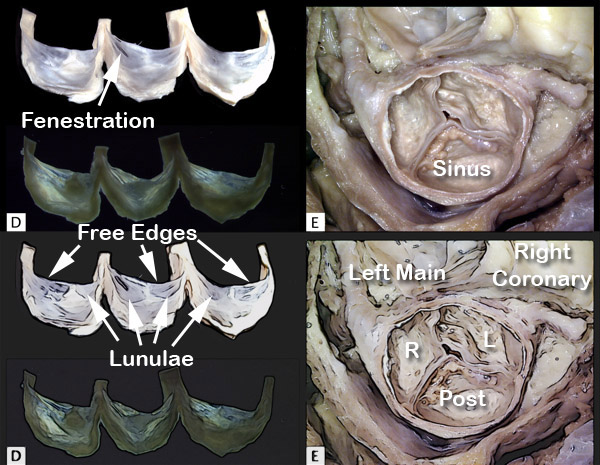 D. The aortic valve cusps of a middle age adult are shown dissected away from the aortic root. The three cusps are thin and delicate with no evidence of fusion. Each cusp shows a central area of fibrous thickening corresponding to the nodule of Arantius. Fenestrations are seen in the lunula of the middle cusp as it reaches the commissure. Examination under polarized light (Lower image in D) shows a collagen weave. E. Degenerative aortic calcification involves the basal regions of the cusps where marked flexion occurs during the cardiac cycle. With progression, the calcific nodules protrude into, and fill the sinuses of Valsalva. The free edges and commissures are not involved. The sinuses are labeled right (R), left (L) and posterior sinus (non-coronary) sinus. The left main coronary artery and the right coronary artery are shown arising from their respective sinuses
D. The aortic valve cusps of a middle age adult are shown dissected away from the aortic root. The three cusps are thin and delicate with no evidence of fusion. Each cusp shows a central area of fibrous thickening corresponding to the nodule of Arantius. Fenestrations are seen in the lunula of the middle cusp as it reaches the commissure. Examination under polarized light (Lower image in D) shows a collagen weave. E. Degenerative aortic calcification involves the basal regions of the cusps where marked flexion occurs during the cardiac cycle. With progression, the calcific nodules protrude into, and fill the sinuses of Valsalva. The free edges and commissures are not involved. The sinuses are labeled right (R), left (L) and posterior sinus (non-coronary) sinus. The left main coronary artery and the right coronary artery are shown arising from their respective sinuses
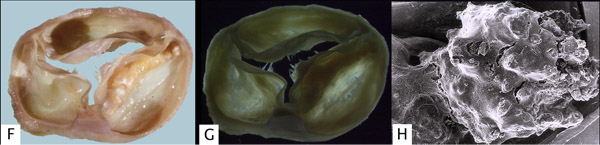 F. Cephalad view of the valve cusps shown in E, but after being dissected away from the heart. In addition to calcification, note the endocardial thickening of the central nodule of Arantius producing small, finger-like projections known as Lambl’s excrescences. G. Examination under polarized light shows an even denser, birefringent collagenous network. The Lambl's excrescences also are birefringent. H. Scanning electron micrograph of the surface of a calcific nodule showing numerous cracks alternating with smooth areas. The latter show endothelial cells with tiny nuclei forming centrally located bulges in the cytoplasm. ( 100 X).
F. Cephalad view of the valve cusps shown in E, but after being dissected away from the heart. In addition to calcification, note the endocardial thickening of the central nodule of Arantius producing small, finger-like projections known as Lambl’s excrescences. G. Examination under polarized light shows an even denser, birefringent collagenous network. The Lambl's excrescences also are birefringent. H. Scanning electron micrograph of the surface of a calcific nodule showing numerous cracks alternating with smooth areas. The latter show endothelial cells with tiny nuclei forming centrally located bulges in the cytoplasm. ( 100 X).